Banner Image Photo: A woman holds a self-sample device for HPV. Credit: Jhpiego/Kate Holt
What is the context? The need for fundamental transformation in our health systems has never been more apparent. Already the world faces a shortage of 13 million health workers. Now, in the context of COVID-19, our dependencies on a stretched health workforce are brought to the fore, demanding creative, urgent, and difficult solutions.
People are asked to steer clear of COVID-19 hotspots such as hospitals and clinics, to use telemedicine or hotlines where they exist, to self-diagnose using symptom guidelines, and to self-medicate. Preventative and curative care jostle together, both equally important, both challenged to be delivered in tandem. World over, millions volunteered almost overnight to support continuity of health services, with clinicians coming out of retirement, and others lending their non-clinical expertise and labor. At individual, community, and health system levels, we are witnessing an overnight transformation in how people use and organize healthcare.
As COVID-19 moved from outbreak to epidemic and now pandemic, and with the significant possibility that for the next 18 months we see episodic outbreaks of COVID-19, one immediate need—and potentially lasting health system transformation—will be learning what services and information can be provided with less dependency on health workers.
These measures are both to protect heroic frontline health workers, but also to ensure the most effective healthcare can be provided at scale. In this context, self-care is not only occurring, but has rapidly become a critical answer in the health system response to COVID-19.
What is self-care? For the uninitiated, the World Health Organization (WHO) defines self-care as “the ability of individuals, families and communities to promote health, prevent disease, maintain health, and cope with illness and disability with or without the support of a healthcare provider,” and add in subsequent publications that “self-care interventions are among the most promising and exciting new approaches to improve health and well-being, both from a health systems perspective and for people who use these interventions.”
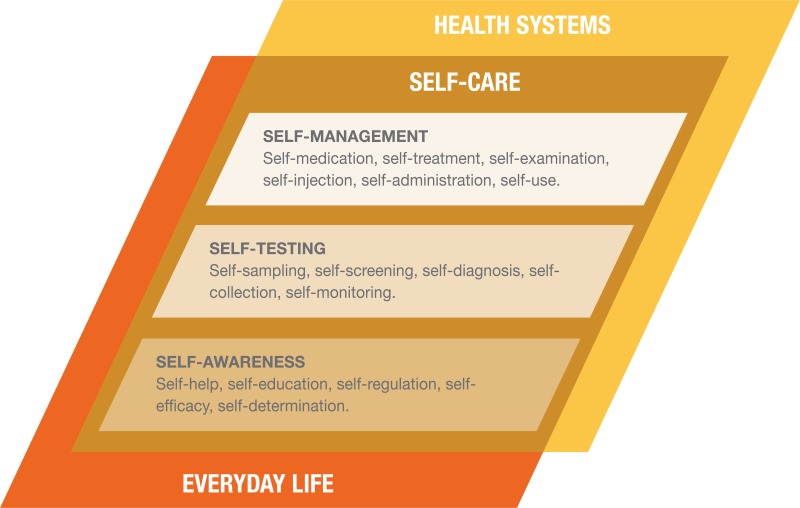
Figure 1. Self-care in the context of interventions linked to health systems.
Source: WHO Consolidated Guideline on Self-Care Interventions for Health
Prior to COVID-19, self-care was already increasing in relevance for health systems. This is not self-care focused on general physical and mental wellness, although self-care does incorporate those broader and important considerations. This is self-care in the form of drugs, diagnostics, devices, and digital health, that—paired with growing demand by individuals for participation in their healthcare—has led to a greater configuration of self-led health care possibilities than ever before. Information, products, and services previously requiring the full participation of health workers have seen individuals take greater responsibility for their health care. Examples of this abound across the range of self-management, self-testing, and self-awareness (see Figure 1). Prior to the outbreak of COVID-19, health systems from Uganda and Nigeria were working on plans to take the 2019 WHO Consolidated Guideline for Self-Care Interventions in Health for Sexual and Reproductive Health and Rights and other self-care interventions to scale. This specific WHO guideline recognizes that many evidence-based practices within the SRHR space could be promoted to enhance self-care, and recommends measures such as HIV self-testing, HPV self-sampling, and self-administered injectable contraception all be available at scale.
Photo: A woman holds a self-sample device for HPV. Credit: Jhpiego/Kate Holt
Why is self-care important in the context of COVID-19? Within a COVID-19 response, self-care is how we help one another, and what keeps our health systems from complete collapse. It appears in our efforts to self-screen through AI-powered websites where we check how common our symptoms are in relation to COVID-19, or in those WHO WhatsApp alerts used to self-educate. It’s the promise of home self-testing (tantalizingly close), and all we do to care for ourselves and our household when someone falls ill.
This sudden and rapid reliance on self-care isn’t how we imagined it—haphazard and driven out of crisis rather than thoughtful health system design. There will be people now managing their health in ways that they should not, cannot, be expected to do alone. In this messiness exist dangers and pitfalls, such as the general public and physicians purchasing and using chloroquine and hydroxychloroquine after recent reports suggested they may be able to treat COVID-19, but with insufficient evidence or reflection on the consequences. The safeguards (financial protection, safe and quality care, adequate support from a health worker when needed) have not been fully established.
But crises don’t wait for us to get it right, as much as they reveal how previously we could have done things differently, better. This leaves us in a transitional moment, where the rapid transformation happening cannot be ignored. Within the lens of outbreak response itself, self-care plays an important function. Self-care will also remain important for the many healthcare needs that carry on regardless of COVID-19. And it will play a critical role in the health systems that exist once the pandemic has subsided.
Photo: An HIV self-test. Credit: Jhpiego/Karen Kasmauski
What does advancing self-care look like? Self-care can mean better, more accessible, participatory, affordable, quality healthcare. In the case of the emergency contraceptive pill or acetaminophen when available over the counter, such self-care will require minimal or no interaction with a health worker. However, frequently, for COVID-19 and many health interventions, self-care requires a carefully choreographed set of interactions between health workers and individuals to enable people to take greater control over their healthcare. As the WHO guidelines also highlight, self-care is not a binary phenomenon of healthcare worker versus person-led healthcare, rather it’s far more dynamic. For example, the HIV self-test may be taken alone but requires referral into the health system for result verification and treatment, if needed. HPV DNA self-sampling allows a woman the control and privacy to collect her own specimens for screening for cervical cancer, but the health system will review the results and assist clients to interpret and act on them, including treatment when applicable. Self-injected DMPA-SC and oral PrEP for HIV prevention might require an initial contact with a pharmacist, clinician, or lay health worker, but are largely used autonomously thereafter—with support provided at intervals to counsel through any adverse effects and adapt regimens or switch methods as needed. The nature of these interactions will vary by intervention, by population, and across people’s lifetimes.
Photo: The DMPA-SC contraceptive method, which can be self-injected. Credit: PSI
What can we do? During the COVID-19 outbreak and beyond, a health system that optimized self-care would therefore consider the following:
It would be designed around continuity of care, including self-care, acknowledging that connections to the health system will often remain and need to be fit for purpose: robust enough to ensure clients receive quality healthcare, yet flexible enough to ensure clients are not prevented from accessing the better healthcare that self-care can provide. Continuity might include use of digital health solutions, such as those being used now to support users at home while protecting healthcare workers from COVID-19.
In addition to a continuity of care approach, such self-care will keep a systematic approach to safety and quality of care front of mind, with processes to ensure technical competence of health workers and people in the delivery of self-care, of client safety and satisfaction, quality information and interpersonal exchanges. The unique role of credible and trusted information is also critical, to address rumors, myths, prevent dangerous practices, and promote good practices.
It would recognize the role of health system actors in promoting and advancing self-awareness—with healthcare workers and individuals not on parallel tracks towards health, but in partnership with one another. This requires healthcare workers take an active role championing health literacy, self-awareness, and promotion of self-care where appropriate. When we’ve been conditioned to view ourselves as recipients of healthcare, it will take healthcare workers to help us shift that paradigm.
Self-care should also keep universal health coverage top of mind, so that access, quality, and equity are not overly compromised amidst the rapid transformation health systems face with this pandemic. In particular, financing of self-care will require as extensive discipline as is applied to the financing of existing health systems, precisely because self-care is a health system solution.
Self-care, enabling people’s own capacity to do what once relied on healthcare workers, would have been one part of the future of healthcare regardless of COVID-19. But to navigate COVID-19 and come out with health systems and public health capacities that are stronger—not further fragmented—it’s increasingly important to find the balance between self-care and what we rely on healthcare workers and health systems to deliver. To the extent possible, documenting and reflecting on this rapid transformation will also be crucial to learning from this. And if there is one ray of hope in challenging times, it is that through necessity, quality self-care may become better organized, resourced, and applied. People, together, can do this.
About the authors This work is co-authored by staff from PSI and Jhpiego. Both organizations are rapidly employing existing and new resources to respond to the COVID-19 pandemic, as well as ensure existing health system capacity is maintained in critical health areas. Through the Self Care Trailblazers Group, generously supported by the Children’s Investment Fund Foundation (UK) and the William and Flora Hewlett Foundation, both PSI and Jhpiego benefit from the collective wisdom and momentum of many organizations working in self-care at global and country level, from FHI 360, PATH, White Ribbon Alliance, IPPF, the Self Care Academic Research Unit at Imperial College London, Johns Hopkins University, SH:24, EngenderHealth, Aidsfonds, Voluntary Service Overseas (VSO) and many others. The technical leadership and support of the World Health Organization has also been vitally important to strengthening the emerging self-care movement, alongside the growing support from the USAID Office of Population & Reproductive Health, the Bill & Melinda Gates Foundation and the UK Department for International Development.
04
Building Resilient, Consumer-Powered Health Systems
PSI’s Health Systems Accelerator is built on 50+ years of experience collecting and elevating consumer and health system insights, scaling innovations and partnering with government and private sector actors to shape stronger, more integrated health systems that work for consumers. Learn more here.
CAN DIGITAL LOCATOR TOOLS IMPROVE ACCESS TO HIGH-QUALITY HEALTH SERVICES AND PRODUCTS IN LOW-RESOURCE SETTINGS?
In the absence of a trusted and dedicated Primary Healthcare (PHC) provider, individuals often spend valuable time and resources navigating through a multitude of health facilities, visiting various providers in search of the right place to address their health concerns. Challenges navigating the health system can result in delays in assessment, diagnosis, and treatment, potentially leading to poor quality of care and adverse health outcomes. One promising solution is the digital locator, which can enable healthcare consumers to promptly find high quality, affordable health products and services when they need them. What are current applications of digital locator tools? How can they be improved? What are the challenges faced in utilizing these tools?
In the ever-evolving health landscape, a robust health management information system (HMIS) stands as a cornerstone of a strong health system. It not only guides decision-making and resource allocation but also shapes the well-being of individuals and communities. However, despite technological advancements that have revolutionized data collection, analytics, and visualization, health systems in low- and middle-income countries (LMICs) continue to grapple with a fundamental challenge: fragmented data and limited effective data use for decision-making. What are some promising solutions?
In this video, Wycliffe Waweru, Head of Digital Health & Monitoring at Population Services International outlines three barriers to the use of data for decision-making in health in low- and middle-income countries. For each barrier, Wycliffe proposes some concrete solutions that can help overcome it.
In this video, Dominic Montagu, Professor Emeritus at the University of California, San Francisco, and CEO of Metrics for Management outlines the three levels of data from private healthcare providers in low- and middle-income countries that need to be sequentially integrated into a country’s health information system to assure that governments can manage the overall health system more effectively.
Join us in this illuminating session as we explore the evolution of the STAR self-testing project, sharing insights, challenges, and successes that have emerged over the years. By examining the lessons learned and considering the implications for future healthcare strategies, we hope to foster a deeper understanding of the transformative potential of self-testing in improving healthcare accessibility and patient-centric services.
This enlightening session promises to provide updates from WHO guidelines and share insights on the journey toward viral hepatitis elimination. It will also showcase outcomes from the STAR hepatitis C self-testing research and discuss how these findings could potentially inform hepatitis B antigen self-testing and the use of multiplex test kits in thecontext of triple elimination. Join us in this crucial discussion as we work together to fast-track the global journey toward a hepatitis-free world by 2030.
In this two-part session, the Bill & Melinda Gates Foundation, PSI, and Population Solutions for Health will share lessons and best practices from rigorous research andhands-on implementation experience in Zimbabwe. The session will cover important topics like client-centered, community-led demand creation, differentiated service delivery, sustainable financing, and digital solutions. The sessions will also cover lessons in the program.
In this session, PSI and PSH will share lessons for optimizing access to comprehensive, culturally sensitive HIV and sexual and reproductive health services. Topics will include enhancing the accuracy and reliability of sex worker population data, improving HIV case finding among men who have sex with men (MSM) through reverse index case testing, and scaling differentiated service delivery models. The session will also cover integrating mental health and substance abuse in key populations (KP) programming and lessons in public sector strengthening.
Additionally, the session will showcase solutions that MSMs have co-designed, highlighting how this collaboration has improved the consumer care experience. It will demonstrate the critical role of KP communities in establishing strong and sustainable HIV responses, including amplifying KP voices, strengthening community-led demand, and establishing safe spaces at national and subnational levels for KP communities to shape and lead the HIV response.
This enlightening session promises to provide updates from WHO guidelines and share insights on the journey toward viral hepatitis elimination. It will also showcase outcomes from the STAR hepatitis C self-testing research and discuss how these findings could potentially inform hepatitis B antigen self-testing and the use of multiplex test kits in the context of triple elimination. Join us in this crucial discussion as we work together to fast-track the global journey toward a hepatitis-free world by 2030.
In this two-part session, the Bill & Melinda Gates Foundation, PSI, and PSH will share lessons and best practices from rigorous research and hands-on implementation experience in Zimbabwe. The session will cover important topics like client-centered, community-led demand creation, differentiated service delivery, sustainable financing, and digital solutions. The sessions will also cover lessons in program management. These insights are applicable beyond Zimbabwe and can be used to scale up HIV prevention efforts in the region.
03
Scaling Digital Solutions for Disease Surveillance
Strong surveillance systems are essential to detect and respond to infectious disease outbreaks. Since 2019, PSI has worked alongside the Ministries of Health in Cambodia, Laos, Myanmar, and Vietnam to strengthen disease surveillance systems and response. Learn more here.
02
Misinformation and Vaccine Hesitancy
As COVID-19 spread globally, so did misinformation about countering the pandemic. In response, PSI partnered with Meta to inspire 160 million people to choose COVID-19 preventative behaviors and promote vaccine uptake. Watch the video to learn how.
01
The Frontline of Epidemic Preparedness and Response
Early warning of possible outbreaks, and swift containment actions, are key to preventing epidemics: disease surveillance, investigation and response need to be embedded within the communities.Public Health Emergency Operations Centers (PHEOCs) are designed to monitor public health events, define policies, standards and operating procedures, and build capacity for disease surveillance and response. Learn more here.
HOW COULD PRIVATE SECTOR PHARMACIES AND DRUG SHOPS ADVANCE PROGRESS TOWARDS UNIVERSAL HEALTH COVERAGE?
Private sector pharmacies and drug shops play an important role in improving access to essential health services and products for millions of people living in low- and middle-income countries (LMICs), where healthcare resources are often limited. However, the way in which these outlets are, or are not, integrated into health systems holds significant importance. Do they serve as facilitators of affordable, high-quality care? Or have they become sources of substandard health services and products?
For over 50 years, PSI’s social businesses have worked globally to generate demand, design health solutions with our consumers, and work with local partners to bring quality and affordable healthcare products and services to the market. Now consolidating under VIYA, PSI’s first sexual health and wellness brand and social business, our portfolio represents the evolution from traditionally donor–funded projects towards a stronger focus on sustainability for health impact over the longterm. Across 26 countries, the VIYA model takes a locally rooted, globally connected approach. We have local staff, partners and providers with a deep understanding of the markets we work in. In 2022, we partnered with over 47,000 pharmacies and 10,000 providers to reach 11 million consumers with products and services, delivering 137 million products. VIYA delivers lasting health impact across the reproductive health continuum, from menstruation to menopause. Consumer insights drive our work from start to finish. Their voices, from product exploration to design, launch, and sales, ensure that products not only meet consumers’ needs but exceed their expectations. The consumer is our CEO.
In 2019, our human-centered design work in East Africa explored ways that our work could support and accompany young women as they navigate the various choices required for a healthy, enjoyable sexual and reproductive life. Harnessing insights from consumers, VIYA is revolutionizing women’s health by addressing the confusion, stigma, and unreliability surrounding sexual wellness. Across five markets – Guatemala, Kenya, South Africa, Uganda and Pakistan – VIYA utilizes technology to provide women with convenient, discreet, and enjoyable tools for making informed choices about their bodies. The platform offers a wealth of high-quality sexual wellness information, covering topics from periods to pleasure in an accessible and relatable manner. Additionally, VIYA fosters a supportive community where users can share experiences and receive guidance from counselors. In 2023, VIYA will begin offering a diverse range of sexual wellness products and connect users with trusted healthcare providers, ensuring comprehensive care tailored to individual needs.
Digitalizing contraceptive counseling to reach rural women and girls in Ethiopia
By: Fana Abay, Marketing and Communications Director, PSI Ethiopia
In rural Ethiopia, women and girls often face significant barriers in accessing healthcare facilities, which can be located hours away. Moreover, there is a prevailing stigma surrounding the use of contraception, with concerns about potential infertility or the perception of promiscuity. To address these challenges, the Smart Start initiative has emerged, linking financial well-being with family planning through clear and relatable messaging that addresses the immediate needs of young couples—planning for the lives and families they envision. Smart Start takes a community-based approach, utilizing a network of dedicated Navigators who engage with women in their localities. These Navigators provide counseling and refer interested clients to Health Extension Workers or healthcare providers within Marie Stopes International-operated clinics for comprehensive contraceptive counseling and services.
In a significant development, PSI Ethiopia has digitized the proven counseling messaging of Smart Start, expanding its reach to more adolescent girls, young women, and couples. This approach aligns with the priorities set by the Ethiopian Ministry of Health (MOH) and is made possible through funding from Global Affairs Canada. The interactive and engaging digital messaging has revolutionized counseling services, enabling clients to make informed and confident decisions regarding both their finances and contraceptive choices.
Clients who received counseling with the digital Smart Start tool reported a higher understanding of their options and were more likely to choose contraception (74 percent) compared to those counseled with the manual version of Smart Start (64 percent). Navigators also found the digital tool more effective in connecting with clients, leading to higher ratings for the quality of their counseling.
By December 2023, PSI Ethiopia, working in close collaboration with the MOH, aims to reach over 50 thousand new clients by leveraging the digital counseling tool offered by Smart Start. This innovative approach allows for greater accessibility and effectiveness in providing sexual and reproductive health services, contributing to improved reproductive health outcomes for women and couples across the country.
Building community health worker capacity to deliver malaria care
By: Christopher Lourenço, Deputy Director, Malaria, PSI Global
Community health workers (CHWs) are critical lifelines in their communities. Ensuring they have the training, support, and equipment they need is essential to keep their communities safe from malaria, especially in the hardest to reach contexts.
For example, in Mali, access to formal health services remains challenging, with four in ten people living several miles from the nearest health center, all without reliable transportation or access. In 2009, the Ministry of Health adopted a community health strategy to reach this population. The U.S. President’s Malaria Initiative (PMI) Impact Malaria project, funded by USAID and led by PSI, supports the Ministry with CHW training and supervision to localize health services.
In 2022, 328 thousand malaria cases were recorded by CHWs); 6.5 thousand severe malaria cases were referred to health centers, according to the national health information system.
During that time, the PMI Impact Malaria project (IM) designed and supported two rounds of supportive supervision of 123 CHWs in their workplaces in the IM-supported regions of Kayes and Koulikoro. This included developing and digitizing a standardized supervision checklist; and developing a methodology for selecting which CHWs to visit. Once a long list of CHW sites had been determined as accessible to supervisors for a day trip (including security reasons), the supervisors telephoned the CHWs to check when they would be available to receive a visit [as being a CHW is not a full-time job, and certain times of the year they are busy with agricultural work (planting, harvesting) or supporting health campaigns like mosquito net distribution].
Supervisors directly observed how CHWs performed malaria rapid diagnostic tests (RDTs) and administered artemisinin-based combination therapy (ACT). They recorded CHW performance using the digitized checklist, interviewed community members, reviewed records, and provided on-the-spot coaching. They also interviewed the CHWs and tried to resolve challenges they expressed, including with resupply of commodities or equipment immediately or soon afterwards.
Beyond the observed interactions with patients, supervisors heard from community members that they were pleased that CHWs were able to provide essential malaria services in the community. And the data shows the impact.
In IM-supported areas of Mali, 36% of CHWs in the first round were competent in performing the RDT, which rose to 53% in the second. 24% of CHWs in the first round compared to 38% in the second were competent in the treatment of fever cases and pre-referral counseling. Between both rounds, availability of ACT increased from 80 percent to 90 percent.
Supportive supervision with interviews and observations at sites improved the basic competencies of CHWs between the first and second rounds, and additional rounds will help to understand the longer-term programmatic benefits.
Taking a market-based approach to scale sanitation in Ethiopia
By: Dr. Dorothy Balaba, Country Representative, PSI Ethiopia
In Ethiopia, PSI leads the implementation of USAID Transform WASH (T/WASH) activity with consortium partners, SNV and IRC WASH. Contrary to traditional models that rely on distribution of free or heavily subsidized sanitation products, T/WASH utilizes a market-based sanitation approach. This approach creates sustainable and affordable solutions, by integrating market forces and supporting businesses to grow, while creating demand at the household level.
During the last six years, T/WASH has worked alongside the private sector and government (Ethiopia’s Ministry of Health, Ministry of Water and Energy, and Ministry of Labor and Skills), among other stakeholders, to increase household access to affordable, quality sanitation products and services. For example, more than 158 thousand households have invested in upgraded sanitation solutions with rapid expansion to come as the initiative scales and market growth accelerates.
T/WASH has successfully trained more than 500 small businesses, including community masons and other construction-related enterprises, with technical know-how in sanitation product installation, operational capacities, and marketing and sales skills needed to run successful, growing businesses. The Ethiopian government is now scaling the approach to all districts through various national, regional, and local institutions with requisite expertise. T/WASH has also worked the One WASH National Program, Ministry of Health, Ministry of Water and Energy, and Ministry of Labor and Skills to examine policies that influence increased household uptake of basic WASH services, such as targeted sanitation subsidies, tax reduction to increase affordability, and increased access to loan capital for business seeking to expand and households needing help to improve their facilities.
To share the journey to market-based sanitation, representatives of the Ethiopian Ministry of Health and the USAID Transform WASH team took to the stage at the UN Water Conference in 2023.
“Rather than relying on traditional aid models that often distribute free or heavily subsidized sanitation products, market-based sanitation creates sustainable and affordable solutions, integrating market forces and supporting businesses to grow.”
— Michael Negash, Deputy Chief Party of T/WASH
Promoting self-managed care like Self-testing and Self-Sampling
By: Dr Karin Hatzold, Associate Director HIV/TB/Hepatitis
Building upon the success and insights gained from our work with HIV self-testing (HIVST), PSI is actively applying this approach to better integrate self-care, more broadly, in the health system beginning with Hepatitis C and COVID-19. Self-testing has emerged as a powerful tool to increase access to integrated, differentiated, and decentralized health services, accelerating prevention, care, and treatment for various diseases, while also increasing health system resilience against COVID-19.
Here’s how we got there.
Seven years ago, the landscape of HIV self-testing lacked global guidelines, and only the U.S., the UK and France had policies in place that allowed for HIV self-testing. High disease burdened countries in low-and-middle-income-countries (LMICs) lacked evidence and guidance for HIVST despite major gaps in HIV diagnosis.
However, through the groundbreaking research from the Unitaid-funded HIV Self-Testing Africa (STAR) initiative led by PSI, we demonstrated that HIVST is not only safe and acceptable but also cost-effective for reaching populations at high risk with limited access to conventional HIV testing. This research played a pivotal role in informing the normative guidelines of the World Health Organization (WHO) and shaping policies at the country level. As a result, more than 108 countries globally now have reported HIVST policies, with an increasing number of countries implementing and scaling up HIVST to complement and partially replace conventional testing services. This became especially significant as nations tried to sustain HIV services amidst the disruptions caused by the COVID-19 pandemic.
By leveraging our expertise, PSI is conducting research to identify specific areas and populations where the adoption of Hepatitis C and COVID-19 self-testing could significantly enhance testing uptake and coverage. This research serves as the foundation for developing targeted strategies and interventions to expand access to self-testing, ensure that individuals have convenient and timely options for testing for these diseases, and are linked to care, treatment and prevention services through differentiated test and treat approaches.
Using peer coaches to counter HIV stigma in South Africa
By: Shawn Malone, Project Director, HIV/AIDS Gates Project in South Africa, PSI Global
In South Africa, where the HIV response has lagged in reaching men, PSI’s Coach Mpilo model has transformed the role of an HIV counselor or case manager into that of a coach and mentor who provides empathetic guidance and support based on his own experience of living with HIV. Coaches are men who are not just stable on treatment but also living proudly and openly with HIV. Situated within the community and collaborating closely with clinic staff, they identify and connect with men struggling with barriers to treatment and support them in overcoming those barriers, whether that means navigating the clinic or disclosing their HIV status to their loved ones.
PSI and Matchboxology first piloted the model in 2020 with implementing partners BroadReach Healthcare and Right to Care as well as the Department of Health in three districts of South Africa. Since then, the model has been rolled out by eight implementing partners in South Africa, employing more than 300 coaches and reaching tens of thousands of men living with HIV. To date, the model has linked 98 percent of clients to care and retained 94 percent of them, in sharp contrast to the estimated 70 percent of men with HIV in South Africa who are currently on treatment.
Given the success of the program, South Africa’s Department of Health and the United States President’s Emergency Plan for AIDS Relief (PEPFAR) have each embraced the Coach Mpilo model in their health strategy and are embedding it in their strategies and programs.
“The men we spoke to [while I was traveling to South Africa for a PrEP project with Maverick Collective by PSI] were not only decidedly open to the idea of taking a daily pill…many were willing to spread the word and encourage friends to get on PrEP too. We were able to uncover and support this new way forward because we had flexible funding to focus on truly understanding the community and the root barriers to PrEP adoption. This is the philanthropic funding model we need to effectively fight the HIV epidemic, and it’s beneficial for all sorts of social challenges.”
– Anu Khosla, Member, Maverick Collective by PSI
simplifying consumers’ journey to care in Vietnam
By: Hoa Nguyen, Country Director, PSI Vietnam
In late 2022, with funding from the Patrick J. McGovern Foundation, PSI and Babylon partnered to pilot AIOI in Vietnam. By combining Babylon’s AI symptom checker with PSI’s health provider locator tool, this digital health solution analyzes symptoms, recommends the appropriate level of care, and points them to health providers in their local area. The main goal is to support people in low-income communities to make informed decisions about their health and efficiently navigate the healthcare system, while reducing the burden on the healthcare workforce. The free 24/7 service saves people time and subsequent loss of income from taking time off work and from having to pay unnecessary out-of-pocket expenses. Under our global partnership with Meta, PSI launched a digital campaign to put this innovative product in the hands of people in Vietnam. By the end of June 2023 (in the nine months since product launch), 210 thousand people accessed the AIOI platform; 2.4 thousand people created personal accounts on the AIOI website, 4.8 thousand triages to Symptom Checker and linked 2.2 thousand people to health facilities.
Babylon’s AI symptom checker and PSI’s health provider locator tool captures real-time, quality data that supports health systems to plan, monitor and respond to consumer and provider needs. But for this data to be effective and useable, it needs to be available across the health system. Fast Healthcare Interoperability Resources (FHIR) standard provides a common, open standard that enables this data exchange. PSI’s first consumer-facing implementation of FHIR was launched in September 2022 as part of the Babylon Symptom Checker project in Vietnam, enabling rapid alignment between PSI and Babylon’s FHIR-enabled client records systems. PSI already has several other consumer health FHIR implementations under active development in 2023, including PSI’s collaboration with the Kenya MOH to launch a FHIR-enabled WhatsApp national health line for COVID-19 health information. PSI will also look to adopt and scale health workforce-facing FHIR-enabled tools, such as OpenSRP2, which will be piloted in an SRH-HIV prevention project in eSwatini in partnership with Ona by the end of 2023.
— Martin Dale, Director, Digital Health and Monitoring, PSI
Engaging the private sector for disease surveillance in Myanmar
By: Dr. Zayar Kyaw, Head of Health Security & Innovation, PSI Myanmar
Under a three-year investment from the Indo-Pacific Center for Health Security under Australia’s Department for Foreign Affairs and Trade (DFAT), PSI is enhancing disease outbreak surveillance and public health emergency preparedness and response capacities in Myanmar, Cambodia, Laos, and Vietnam. When PSI conducted a review of existing disease surveillance systems in Myanmar, it identified several gaps: although the Ministry of Health had systems in place for HIV, tuberculosis, malaria and other communicable diseases, they were fragmented, with different reporting formats and reliance on paper-based reporting. In addition, private sector case surveillance data were not routinely captured, yet private clinics and pharmacies are the dominant health service delivery channel in the country. This hindered effective disease prevention and control efforts.
Building on our extensive private sector malaria surveillance work under the BMGF-funded GEMS project in the Greater Mekong Subregion, PSI implemented a case-based disease notification system using social media channels to overcome the limitations of paper-based and custom-built mobile reporting tools. These chatbots, accessible through popular social media platforms like Facebook Messenger and Viber, proved to be user-friendly and required minimal training, maintenance, and troubleshooting. The system was implemented in more than 550 clinics of the Sun Quality Health social franchise network as well as nearly 470 pharmacies. The captured information flows to a DHIS2 database used for real-time monitoring and analysis, enabling rapid detection of potential outbreaks. Local health authorities receive instant automated SMS notifications, enabling them to promptly perform case investigation and outbreak response.
In 2022, private clinics reported 1,440 malaria cases through the social media chatbots, while community mobilizers working with 475 private providers and community-based malaria volunteers reported more than 5,500 cases, leading to the detection of two local malaria outbreaks. Local health authorities were instantly notified, allowing them to take action to contain these surges in malaria transmission. During the same time, pharmacies referred 1,630 presumptive tuberculosis cases for confirmatory testing – a third of which were diagnosed as tuberculosis and enrolled into treatment programs.
Training health workers in Angola
By: Anya Fedorova, Country Representative, PSI Angola
The shortage of skilled health workers is widely acknowledged as a significant barrier to achieving Universal Health Coverage. To address this challenge, PSI supported ministries of health to develop a digital ecosystem that brings together stewardship, learning, and performance management (SLPM). The ecosystem enhances training, data-driven decision-making, and the efficiency of healthcare delivery.
Here’s what it looks like in practice.
In July 2020, PSI Angola, alongside the Angolan digital innovation company Appy People, launched Kassai, an eLearning platform that targets public sector health workers in Angola. Through funding from USAID and the President’s Malaria Initiatve (PMI), Kassai features 16 courses in malaria, family planning, and maternal and child health – with plans to expand learning topic areas through funding from ExxonMobil Foundation and private sector companies. A partnership with UNITEL, the largest telecommunication provider in Angola, provides all public health providers in Angola free internet access to use Kassai.
Kassai’s analytics system to follow learners’ success rate and to adjust the course content to learners’ performance and needs. Kassai analytics are integrated with DHIS2 – the Health Management Information System (HMIS) of Angolan MOH, to be able to link learners’ knowledge and performance with the health outcomes in the health facilities. The analytics track learners’ performance by course and gives visibility by health provider, health facility, municipality, and province. Each course has pre-and post-evaluation tests to track progress of learning, too.
By the end of 2022, there were 6,600 unique users on the Kassai platform and 31,000 course enrollments. PSI Angola’s partnership with UNITEL, the largest telecommunication provider in Angola, allows for free internet access to learn on the Kassai for all public health providers in Angola. Building on its success for malaria training, Kassai now also provides courses in family planning, COVID-19, and maternal and child health. This reduces training silos and provides cross-cutting benefits beyond a single disease.
Implementing the SLPM digital ecosystem brings numerous benefits to health systems. It allows for more strategic and efficient workforce training and performance management, enabling ministries of health to track changes in health workers’ knowledge, quality of care, service utilization, and health outcomes in real time. The ecosystem also supports better stewardship of mixed health systems by facilitating engagement with the private sector, aligning training programs and standards of care, and integrating private sector data into national HMIS. Furthermore, it enables the integration of community health workers into the broader health system, maximizing their impact and contribution to improving health outcomes and strengthening primary healthcare.
OUR COMMITMENTS
WHISTLEBLOWER AND ANTI-RETALIATION
PSI does not tolerate retaliation or adverse employment action of any kind against anyone who in good faith reports a suspected violation or misconduct under this policy, provides information to an external investigator, a law enforcement official or agency, or assists in the investigation of a suspected violation, even if a subsequent investigation determines that no violation occurred, provided the employee report is made in good faith and with reasonable belief in its accuracy.
PSI’s code sets out our basic expectations for conduct that is legal, honest, fair, transparent, ethical, honorable, and respectful. It is designed to guide the conduct of all PSI employees—regardless of location, function, or position—on ethical issues they face during the normal course of business. We also expect that our vendors, suppliers, and contractors will work ethically and honestly.
With overarching commitments to flexibility in our work, and greater wellbeing for our employees, we want to ensure PSI is positioned for success with a global and holistic view of talent. Under our new “work from (almost) anywhere,” or “WFAA” philosophy, we are making the necessary investments to be an employer of record in more than half of U.S. states, and consider the U.S. as one single labor market for salary purposes. Globally, we recognize the need to compete for talent everywhere; we maintain a talent center in Nairobi and a mini-hub in Abidjan. PSI also already works with our Dutch-based European partner, PSI Europe, and we’re creating a virtual talent center in the UK.
OUR COMMITMENTS
Meaningful Youth Engagement
PSI is firmly committed to the meaningful engagement of young people in our work. As signatories of the Global Consensus Statement on Meaningful Adolescent & Youth Engagement, PSI affirms that young people have a fundamental right to actively and meaningfully engage in all matters that affect their lives. PSI’s commitments aim to serve and partner with diverse young people from 10-24 years, and we have prioritized ethics and integrity in our approach. Read more about our commitments to the three core principles of respect, justice and Do No Harm in the Commitment to Ethics in Youth-Powered Design. And read more about how we are bringing our words to action in our ICPD+25 commitment, Elevating Youth Voices, Building Youth Skills for Health Design.
OUR COMMITMENTS
Zero Tolerance for Modern-Day Slavery and Human Trafficking
Since 2017, PSI has been a signatory to the United Nations Global Compact, a commitment to align strategies and operations with universal principles of human rights, labor, environment and anti-corruption. Read about PSI’s commitment to the UN Global Compact here.
Affirmative Action and Equal Employment Opportunity
PSI does not discriminate against any employee or applicant for employment because of race, color, religion, sex, sexual orientation, gender identity, national origin, age, marital status, genetic information, disability, protected veteran status or any other classification protected by applicable federal, state or local law. Read our full affirmative action and equal employment opportunity policy here.
OUR COMMITMENTS
Zero Tolerance for Discrimination and Harassment
PSI is committed to establishing and maintaining a work environment that fosters harmonious, productive working relationships and encourages mutual respect among team members. Read our policy against discrimination and harassment here.
PSI is committed to serving all health consumers with respect, and strives for the highest standards of ethical behavior. PSI is dedicated to complying with the letter and spirit of all laws, regulations and contractual obligations to which it is subject, and to ensuring that all funds with which it is entrusted are used to achieve maximum impact on its programs. PSI provides exceptionally strong financial, operational and program management systems to ensure rigorous internal controls are in place to prevent and detect fraud, waste and abuse and ensure compliance with the highest standards. Essential to this commitment is protecting the safety and well-being of our program consumers, including the most vulnerable, such as women and children. PSI maintains zero tolerance for child abuse, sexual abuse, or exploitative acts or threats by our employees, consultants, volunteers or anyone associated with the delivery of our programs and services, and takes seriously all complaints of misconduct brought to our attention.
OUR FOCUS
Diversity and Inclusion
PSI affirms its commitment to diversity and believes that when people feel respected and included they can be more honest, collaborative and successful. We believe that everyone deserves respect and equal treatment regardless of gender, race, ethnicity, age, disability, sexual orientation, gender identity, cultural background or religious beliefs. Read our commitment to diversity and inclusion here. Plus, we’ve signed the CREED Pledge for Racial and Ethnic Equity. Learn more.
We prioritize the voices of people and communities in designing programs, deliver direct-to-consumer products and information, and accelerate social and behavioral change for health impact.
Across 40+ countries, we scale digital solutions that make it easier for people to take ownership of their own health, and health systems to use resources efficiently and increase health impact.
Supporting People to be Active Agents in their Healthcare
We support health systems in shaping the policy and regulatory environment for self-care interventions and ensuring self-care is included as an essential part of healthcare services.